
More Information
Submitted: 29 November 2019 | Approved: 04 December 2019 | Published: 05 December 2019
How to cite this article: Liu M, Wu K, Tan Y. Localized intrapulmonary desmoplastic mesothelioma: A case report. J Radiol Oncol. 2019; 3: 014-016.
DOI: 10.29328/journal.jro.1001030
Copyright License: © 2019 Liu M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Lung; Desmoplastic; Mesothelioma; Tomography; X-ray computed
Abbreviations: DMM: Desmoplastic Malignant Mesothelioma; CT: Chest computed Tomography; SFT: Solitary Fibrous Tumor

Localized intrapulmonary desmoplastic mesothelioma: A case report
Meng Liu, Kaifu Wu and Yongming Tan*
Department of Health, The First Affiliated Hospital of Nanchang University, China
*Address for Correspondence: Yongming Tan, Master’s Degree, Department of Radiology, The First Affiliated Hospital of Nanchang University, 17 Yongwaizheng Street, Nanchang, Jiangxi, 330006, China, Tel: +86 15179108696; Email: [email protected]
Introduction: Desmoplastic Malignant Mesothelioma (DMM) is a rare histological subtype of sarcomatoid malignant mesothelioma arising most frequently in the pleura or peritoneum and less frequently in the lung parenchyma.
Patient concerns: A 52-year-old female with no apparent asbestos exposure was referred for consultation in our center after 1 month of cough and no concomitant symptoms of chest.
Diagnosis: Chest computed Tomography (CT) revealed a localized mass measuring 4.5 x 3.9 cm in the right lung middle lobe with inhomogeneous enhancement following injection of contrast, and without pleural lesions, considered a primary intrapulmonary desmoplastic mesothelioma.
Interventions: Surgical intervention was performed.
Outcomes: Following complete tumor resection, the patient declined to receive chemotherapy or radiotherapy. The final diagnosis of intrapulmonary desmoplastic mesothelioma was confirmed by pathological and immunohistochemical examination. In addition, no local tumor recurrence was observed within 10 months of follow-up.
Conclusion: Even elderly female patients with localized pulmonary masses without significant pleural lesions should not excluded the possibility of malignant mesothelioma in the lungs.
Desmoplastic mesothelioma typically represents an extremely rare histological subtype of sarcomatoid malignant mesothelioma that usually presents with a diffuse pattern of growth [1] and is commonly found in the pleura and peritoneum. The case of localized intrapulmonary desmoplastic mesothelioma is especially rare, although few cases of true intraparenchymal mesothelioma arising in lung have been described [2,3]. It is difficult to diagnose these tumors clinically and radiologically, and they can finally be confirmed through pathological examination with immunohistochemistry. The current study reports a case of primary intrapulmonary desmoplastic mesothelioma characterized by a localized mass and without pleural invasion. In addition, the clinical and pathological features of this unusual tumor are included. Written informed consent was obtained from the patient’s family.
A 52-year-old female consult to the First Affiliated Hospital of Nanchang University (Jiangxi, China) in December 2016 who presented with cough for one month. This patient has no concomitant symptoms of chest (no expectoration and hemoptysis, no fever, no chest pain). The physical examination showed no abnormality, and routine hematological and biochemical parameters were within normal range. The cough without obvious predisposing causes and the patient had not a clear history of asbestos exposure. Anti-infective therapy (Penicillin, intravenous infusion, 2 million to 10 million UU daily) without improvement after one week.
Chest CT scan showed a mass measuring 4.5 x 3.9 cm in the right lung middle lobe with inhomogeneous enhancement (Figure 1A-E). Based on these findings, an intrapulmonary tumor such as an inflammatory granuloma or lung cancer was suspected.
Exploratory thoracotomy showed a mass measuring 6 x 5 x 4 cm in the right lung middle lobe, without pleural invasion and palpable mediastinal lymph nodes, which the mass tissue is firm and rubbery macroscopically.
Histological findings showed proliferated atypical mesothelial cells and at least half consisted of irregular, dense, hyalinized collagen fibers. These tumor cells with consistent size and shape were arranged into various forms (tubular and papillary pattern eg.) (Figure 1F). Desmoplastic mesothelioma was suspected.
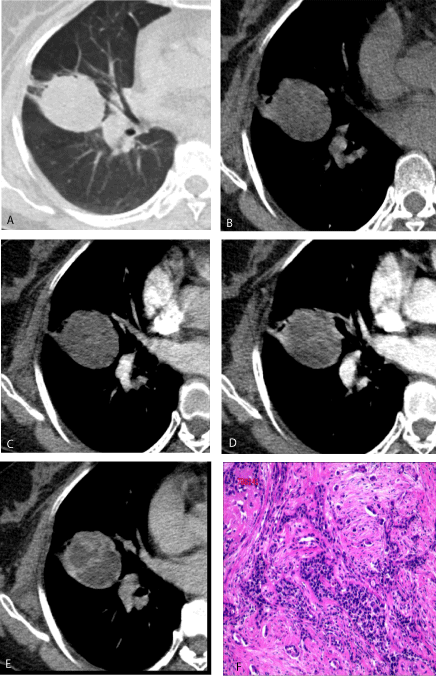
Figure 1: Ulcerative ungual exostosis of the big toe (the tumor is centrally developing, lifting and deforming the nail).
Immunohistochemical analysis revealed that the tumor was positive for calretinin, D2-40, cytokeratin, cytokeratin-5/6, vimentin, calponin, Epithelial membrane antigen, Neuron-specific enolase and Ki-67 (1%), and negative results for Thyroid transcription factor-1, Carcino-embryonic antigen, cytokeratin 7, NapsinA, P63, CD56, desmin, Smooth muscle actin, actin and CD68. By all these histomorphological and immunohistochemical findings, intrapulmonary desmoplastic mesothelioma was confirmed.
The patient had not received chemotherapy or radiotherapy after surgery. As of the time of writing, 10 months postoperatively, the patient has shown no disease recurrence.
Our study was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University, and the family members of the patient have provided informed consent for the publication of the case.
Desmoplastic mesothelioma is a relatively rare histological subtype of mesothelioma with sarcomatoid histology (1) arising most frequently in the pleura, peritoneum or pericardium and less frequently in organs such as lung, spleen [4], pancreas [5] and liver [6]. In fact, few cases of intrapulmonary malignant mesothelioma have been described [2,3,7,8] presenting with bilateral miliary pulmonary nodules and diffuse bilateral opacities or characterized by diffuse intrapulmonary growth, among which some cases [7,8] were pathologically confirmed as intrapulmonary metastases from a clinically undetectable pleural mesothelioma, while the others [2,3] were diagnosed as diffuse intrapulmonary malignant mesothelioma. However, we described an unusual presentation of intrapulmonary mesothelioma characterized by a localized mass without pleural lesions. Clinically and radiologically, the current patient was first diagnosed as pulmonary inflammatory granuloma or lung cancer. The final diagnosis of intrapulmonary DMM was confirmed through pathological examination with immunohistochemistry. To the best of our knowledge, there is no previous report of an intrapulmonary desmoplastic mesothelioma presenting as a localized mass without pleural invasion in literature. And it is difficult to make a definitive pre-operative diagnosis in such case.
Sonja Klebe, et al. [9] reviewed 326 sarcomatoid malignant mesotheliomas with 70 cases (21%) classified as DMM and without a case arising in lung and found it occurred more commonly in men. In addition, although mesothelioma is clearly associated with asbestos exposure, the association between DMM and asbestos exposure is controversial [10]. However, the current female patient had not been exposed to asbestos. Patient with DMM typically present with pleural effusion and pleural thickening [11] and are more frequently associated with metastases compared with other series of mesothelioma [12]. However, the current case was presented with a localized mass in the lung parenchyma without distant metastases and marked pleural invasion.
Histologically, DMM is characterized by at least 50% of the tumor consisting of dense, hypocellular collagenous tissue, with paucicellular atypical mesothelial proliferation [11]. It is essential to differentiate intrapulmonary DMM from other pulmonary tumors, such as sarcomatoid carcinoma, because of important differences in treatment and prognosis. Pathological diagnosis is the most reliable diagnostic method. And immunohistochemical staining can aid in making the diagnosis by providing additional characteristic histological information, in that DMM is positive for calretinin and D2-40, but negative for Carcino-embryonic antigen and other carcinoma related markers [13]. Furthermore, pulmonary sarcomatoid carcinoma usually presents as a peripheral mass, especially located at the apex of the lung.
Other differential diagnosis: (1) Solitary Fibrous Tumor (SFT) have the basic features of benign tumors, Such as round solitary masses with smooth edges. Mixed different proportions of fusiform tumor cells and collagen components histologically adding necrosis, cystoid and mucoid degeneration diffuse distribution, so that enhancement of SFT in arterial phase is not obvious but obvious in the venous phase, which is the characteristic of progressive enhancement. (2) Inflammatory myofibroblastoma of lung: This tumor density was not uniform, so its liquefaction, necrosis, obviously enhancement are common imaging findings.
Currently, DMM without definitive treatment is generally managed according to mesothelioma guidelines. And National Comprehensive Cancer Network guidelines recommend that patient with malignant mesothelioma should receive chemotherapy [14]. In addition, sarcomatoid mesotheliomas are associated with an especially poor prognosis [9], with the median survival time of 3.8 months for DMM patients [11]. However, the current patient was treated without chemotherapy and underwent surgery, and 10 months postoperatively, the patient has shown no local recurrence.
In conclusion, the probability of intrapulmonary malignant mesothelioma should not be ruled out, even in an old female patient presented with pulmonary localized mass without marked pleural lesions.
- Galateau-Salle F, Churg A, Roggli V, Travis WD, World Health Organization Committee for Tumors of the Pleura. The 2015 World Health Organization Classification of Tumors of the Pleura: Advances since the 2004 Classification. J Thorac Oncol. 2016; 11: 142-154. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/26811225
- Hida T, Hamasaki M, Matsumoto S, Abe S, Takakura K, et al. Diffuse intrapulmonary malignant mesothelioma presenting with miliary pulmonary nodules: A case report. Pathol Int. 2015; 65: 318-323. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25759091
- Larsen BT, Klein JR, Hornychová H, Nuti R, Thirumala S. Diffuse intrapulmonary malignant mesothelioma masquerading as interstitial lung disease: a distinctive variant of mesothelioma. Am J Surg Pathol. 2013; 37: 1555-1564. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/23797722
- Giansanti M, Bellezza G, Guerriero A, Pireddu A, Sidoni A. Localized Intrasplenic Mesothelioma: A Case Report. Int J Surg Pathol. 2014; 22: 451-455. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/24050959
- Espinal-Witter R, Servais EL, Klimstra DS, Lieberman MD, Yantiss RK. Localized intrapancreatic malignant mesothelioma: a rare entity that may be confused with other pancreatic neoplasms. Virchows Arch. 2010; 456: 455-461. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20148337
- Serter A, Buyukpinarbasili N, Karatepe O, Kocakoc E. An unusual liver mass: primary malignant mesothelioma of the liver: CT and MRI findings and literature review. Jpn J Radiol. 2015; 33: 102-106. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25518822
- Hasegawa M, Sakai F, Sato A, Tsubomizu S, Arimura K, et al. FISH analysis of intrapulmonary malignant mesothelioma without a clinically detectable primary pleural lesion: an autopsy case. Jpn J Clin Oncol. 2014; 44: 1239-1242. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25425731
- Rossi G, Cavazza A, Turrini E, Costantini M, Casali C, et al. Exclusive intrapulmonary lepidic growth of a malignant pleural mesothelioma presenting with pneumothorax and involving the peritoneum. Int J Surg Pathol. 2006; 14: 234-237. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16959711
- Klebe S, Brownlee NA, Mahar A, Burchette JL, Sporn TA, et al. Sarcomatoid mesothelioma: a clinical-pathologic correlation of 326 cases. Mod Pathol. 2010; 23: 470-479. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20081811
- Ishikawa R, Kikuchi E, Jin M, Fujita M, Itoh T, et al. Desmoplastic malignant mesothelioma of the pleura: autopsy reveals asbestos exposure. Pathol Int. 2003; 53: 401-406. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/12787316
- Hashimoto K, Okuma Y, Hosomi Y, Hishima T. Malignant mesothelioma of the pleura with desmoplastic histology: a case series and literature review. BMC cancer. 2016; 16: 718. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27599565
- Cantin R, Al-Jabi M, McCaughey WT. Desmoplastic diffuse mesothelioma. Am J Surg Pathol. 1982; 6: 215-222. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/7102900
- Husain AN, Colby TV, Ordóñez NG, Allen TC, Attanoos RL, et al. Guidelines for pathologic diagnosis of malignant mesothelioma: 2012 update of the consensus statement from the International Mesothelioma Interest Group. Arch Pathol Lab Med. 2013; 137: 647-667. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28686500
- Ettinger DS, Wood DE, Akerley W, Bazhenova LA, Borghaei H, et al. NCCN Guidelines Insights: Malignant Pleural Mesothelioma, Version 3.2016. J Natl Compr Canc Netw. 2016; 14: 825-836. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27407123